![]() You don't need to be an 'investor' to invest in Singletrack: 6 days left: 95% of target - Find out more
You don't need to be an 'investor' to invest in Singletrack: 6 days left: 95% of target - Find out more
Here's the objective of the 2013 NHS property grab finally revealed
NHS organisations are now going to have to pay full market rental rates on property it previously owned.
http://www.property.nhs.uk/what-we-do/charges1617/
Good luck finding a GP or Community Hospital in London, once the 12 months of transition funding dries up
All done in the best possible taste since
"It drives better and more efficient use of space." FFS
And just tweak those thumbscrews a little more, not enough of us are complaining. Or complaining in the right way, if there is a right way to complain?
Seems sensible, should help them make better use of facilities and/or move usage of space to cheaper locations.
Why should a publicly owned health service - run for the good of all - have to compete with private business?Seems sensible, should help them make better use of facilities and/or move usage of space to cheaper locations.
So you end up with the property developer buying the land, demolishing it and rebuilding apartments. We now have a few more properties at the top of the price ladder.
Then you have to build a new hospital in a new location (which isn't chosen on convenience of location, but cost).
What have you gained?
move usage of space to cheaper locations.
london NHS: outside the m25 since 2017
Seems sensible, should help them make better use of facilities and/or move usage of space to cheaper locations.
Great, just relocate all the GP surgeries in London to Hull, that will work!
[i]Why should a publicly owned health service - run for the good of all - have to compete with private business?[/i]
Who says they have to compete? What matters is that they are using 'space' efficiently, how many buildings has the NHS in Central London for example that are underused and/or don't need to be there?
Seems they've 500 buildings and 400 folk managing the portfolio:
http://www.property.nhs.uk/about-us/regional-and-local-focus/london/
It'll be fine, we just need to leave the EU and the NHS will be miraculously fixed and everyone in hospital will be cured (according to that "advert" on telly.......... ) 😆
You really believe that "What matters is that they are using 'space' efficiently
Cause I thought what mattered was "care of patients" . But heyho diverting £60million away from care to estate agents sounds sensible.
It's perfectly obvious that this is all about, removing the pre-tax loss of £480m made by NHS Property Services Ltd. (year to March 2015.) and making it more attractive, to a full private sector sell-off
Our local hospital now has outpatient services at local gp surgerys, reducing amount of patients attending hospital just for a follow up chat, and progress report, seems to work ok.
y, how many buildings has the NHS in Central London for example that are underused and/or don't need to be there?
Dont know have you an answer? I assume there is some research somewhere....have you seen it?
maxtorque - MemberIt'll be fine, we just need to leave the EU and the NHS will be miraculously fixed and everyone in hospital will be cured (according to that "advert" on telly.......... )
I wasn't in the room but I'm sure they said with the money we save from not being in the EU we could build a hospital a week.
So that will be more empty buildings 🙄 Not sure where the staff fit in with this as once out of the EU Johnny Foreigner will have to jump through hoops of burning straw to bring their skills to work in the NHS
Well how about someone does an audit of space use then. All this is going to do it put more financial pressure on the NHS. It's a cut trying to look like something else.Who says they have to compete? What matters is that they are using 'space' efficiently, how many buildings has the NHS in Central London for example that are underused and/or don't need to be there?
We've just downsized our office space to meet the new government space efficiency programme. And don't get me wrong, there was space to waste. So we got rid of it. But within 3 months a different efficiency project decided to close other offices in the region and make us the hub. So we have had to rent back some of the space we had just given up. Guess what? The rents gone up!
I'm all for efficiency, there are still things that could be improved in the public sector.
Problem is, the people making the decisions don't know what they are. Or care. And the cuts,and the resulting poor decisions,will just keep on coming, and people's lives will be ruined, and some will die, one way or another, as a result.
I'm a naturally right leaning political animal, but both MrsMC and I work in different parts of the public sector, and what we see every day is really concerning.
Not sure where the staff fit in with this as once out of the EU Johnny Foreigner will have to jump through hoops of burning straw to bring their skills to work in the NHS.
MrOvershoot - Who says that will be the case? I could walk into a nursing job in the US/Canada or Australia, all countries with fairly strict immigration controls. Why? Because countries who require certain skilled labour allow such labour in. Given the the [url= http://www.who.int/mediacentre/news/releases/2013/health-workforce-shortage/en/ ]World Health Organisation predicted a few years back[/url] that things are only going to get worse then, in or out of the EU, the ability for overseas nurses to get NHS jobs is very unlikely to change.
And no, I'm not some rabid Leave campaigner, just someone a little tired of the absurd "the world will end" rhetoric being pumped out by both sides.
This isn't "another nail in the coffin", it's a sensible and long overdue reform of NHS land use.
Successive governments have tried and failed to encourage the NHS to release some of its redundant real estate for redevelopment. One of the major constraints on tackling the shortage of housing in cities is the lack of access to land / sites by developers - something Labour have also recognised per the recent pronouncements by Sadiq Khan amongst others.
Dealing with individual PCTs (as was) was a complete non starter for most developers - many NHS "Estate Managers" have little / no experience but view themselves as would be commercial property developers and are either unable to negotiate terms to release land or enter into contacts that are very poor value for the public. This is why 13% of the available land was put under one single body to try and speed the process up and make it easier for developers to find land in the first place.
Some random trivia:
- The NHS owns more land than the space occupied by the City of Derby
- In London the NHS owns land equivalent to 3 x the size of Hyde Park
- Between 15% (acute trusts) and 20% (mental health) of all the land owned by the NHS is unutilised
- Space utilisation is poor by international comparators - with savings of up to 30% in the estate that the NHS does use
- The NHS has amongst the highest spending on estates / buildings in Europe but the lowest spend on medical equipment
It's also worth noting that length of stays are dramatically shorter for many conditions that 30-40 years ago when many Hospitals were built - so we need less hospitals and less beds in hospitals. As a society we have quite a simple choice - either carry on wasting money maintaining buildings that are underused and cost a lot to run and maintain, or remove this spare capacity and return the funds to the NHS for long overdue capital investment.
Anyone who has toured NHS hospitals won't have failed to notice that most have large single story car parks. The fact that the NHS can't even organise multi story parking to free up land is symptomatic of the lack of accountability for one of the most valuable land banks in the country - the other good example being Network Rail.
Plenty more here:
- The NHS owns more land than the space occupied by the City of Derby
- In London the NHS owns land equivalent to 3 x the size of Hyde Park
What is this "Derby" and "hyde park" guff?
Everyone knows that the convention is to express these figures in terms of Olympic swimming pools, St Paul's Cathedral or Wales.
sootyandjim - MemberAnd no, I'm not some rabid Leave campaigner, just someone a little tired of the absurd "the world will end" rhetoric being pumped out by both sides.
Sorry if I upset you, like you I'm fed up with both sides in the way they present the argument & I would probably have made a similar post the other way.
It's just this build hospitals line that gets me without the staff, as I am sure you probably know better than me how difficult it is to fill posts.
we need less hospitals and less beds in hospitals
[img] 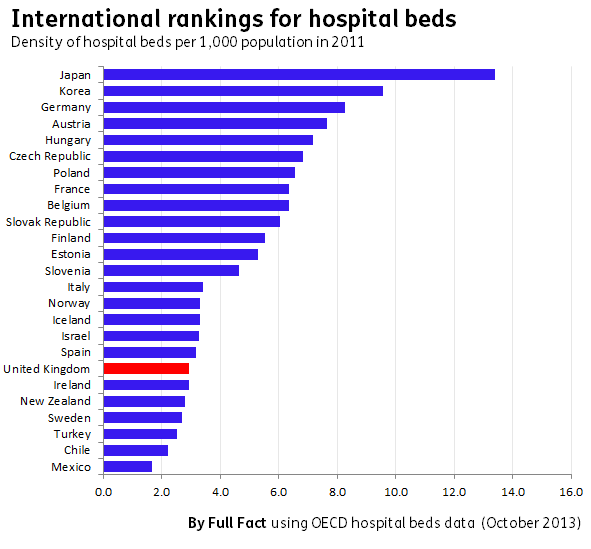 [/img]
[/img]
[img]  [/img]
[/img]
One of the major constraints on tackling the shortage of affordable housing in cities is the lack of access to funds by local authorities
FTFY
Plenty of housing in London, question is - how high do you want to go?
just5minutes - Member- The NHS has amongst the highest spending on estates / buildings in Europe but the lowest spend on medical equipment
That'll certainly be resolved by increasing those costs.
It's just this build hospitals line that gets me without the staff, as I am sure you probably know better than me how difficult it is to fill posts.
MrOvershoot - I have current, real experience on how difficult it is to fill vacancies in hospitals and yes, if we did "build a hospital a week" (the Leave campaign have said we could, not we would) on what we may or may not save by leaving the EU, they would be difficult to staff. That isn't what I took issue with your statement over though.
The Emergency Admissions Unit I work on is staffed about a third with nurses from Portugal and Spain. Leaving the EU wouldn't mean that suddenly we couldn't recruit nurses from there. The UK (as the US, Canada, Australia, etc) could very well say "we need nurses, so registered nurses will be given preferential treatment to move to the UK". It's not some sort of complex issue. The government identifies a particular skill shortage in its workforce and allows preferential recruitment.
The NHS owns more land than the space occupied by the City of Derby
- In London the NHS owns land equivalent to 3 x the size of Hyde Park
That's fascinating, but please explain how its in any way relevant with 60 million people to look after I'm sure that they need some space
- Between 15% (acute trusts) and 20% (mental health) of all the land owned by the NHS is unutilised
And yet there's an acute bed shortage especially in mental health, slashed council budgets unable to take up the care they are supposed to be
http://www.theguardian.com/society/2016/feb/09/mental-health-patients-travel-across-uk-for-beds
- Space utilisation is poor by international comparators - with savings of up to 30% in the estate that the NHS does use
It' also worth noting that length of stays are dramatically shorter for many conditions that 30-40 years ago when many Hospitals were built - so we need less hospitals and less beds in hospitals. As a society we have quite a simple choice - either carry on wasting money maintaining buildings that are underused and cost a lot to run and maintain, or remove this spare capacity and return the funds to the NHS for long overdue capital investment
Shirley with an ageing population this is madness, as the NHS is pressured further they would be forced to rent out or buy the space back as the need increases at inflated prices.
I'm sure plenty of space could be used better by the NHS
Trying to blame it for the housing crisis is a bit much
There's over half a million homes could be built tomorrow, but property companies sit on the land until the prices rise.
There's also the issue of skilled labourer shortage, which could really get due if we leave the EU
. The UK (as the US, Canada, Australia, etc) could very well say "we need nurses, so registered nurses will be given preferential treatment to move to the UK". It's not some sort of complex issue. The government identifies a particular skill shortage in its workforce and allows preferential recruitment.
As Someone who has to arrange visas for students and staff to come and work in our university I can confirm that it is much harder, slower , frustrating and more expensive to recruit from outside the EU than from within, in not sure the NHS needs a shitload more redtape dumped on it
@ernie a perfect example of population growth via immigtation is impacting our services. Each year we add 350,000 people via immigration - how many new hospitals do we have to build for them ?
Also as I posted on the other hread we need a serious conversation about Health service provision as we need to spend much mkre money. Much more.
Royal Brompton and Marsden - do these facilities really have to be in the center of Chelsea ?
The Marsden and the ICR has a much bigger site at Sutton.
I'm not sure what the benefit of a specialist cancer centre would be having it on or out of the M25,
I do know the fundraisers would be very disappointed if they had to do their prestige tours at Sutton, rather than in Chelsea tho
I'm sure you could make the same arguments about Imperial and UCL, too
I doubt it would benefit them to move either
jambalaya - Member@ernie a perfect example of population growth via immigtation is impacting our services.
You mean a perfect example of how the UK has less beds per 1,000 population than the average for other comparable countries, despite the claim made by J5M that we have too many hospital beds.
And you provide a perfect example of how right-wingers use every opportunity to make petty xenophobic points.
.
kimbers - MemberThere's also the issue of skilled labourer shortage, which could really get due if we leave the EU
I don't know why you think controlled immigration means no immigration, or why you think immigration is the only solution to skills shortages.
I agree ernie, but as pointed out from my own experiences, controls mean extra costs in time and money to the employer.
With our current bumper immigration failing to meet demand, I don't see how a restricted version will help
re "Successive governments have tried and failed to encourage the NHS to release some of its redundant real estate for redevelopment."
You must have missed the 1980s when virtually all of the Psychiatric Hospitals were closed and sold off for housing
re: This is why 13% of the available land was put under one single body to try and speed the process up and make it easier for developers to find land in the first place.
Wow even better. So the NHS needs to be reformed for the benefit of property developers. Lets just hope the punishing market rental costs incurred on land in London that the [u]NHS previously owned[/u] is going to teach it a real lesson and really kicks off another proper oligarch feeding frenzy
P.S its only - "Since 2010, national planning policy no longer imposes [u]maximum[/u] parking standards on development, and no longer recommends the use of car parking charges as a demand management measure to discourage car use"
So you want Hospital Trusts to have started building multi-storey car-parks (which take decades to break ££s even) at a time when the NHS overspend is at an all time high ?. Especially when the car-park management and revenue collection has virtually all been outsourced. ?
Doesn't 'bed' usually refer to a treatment capability, not an actual bed?
And FFS people it's FEWER beds not less beds! ARGH!
@ernie I think the NHS is massively underfunded (beds included). We need politians to admit that what we have doesn't need saving - it needs a massive upgrade and imo a redesign. Plus they need ro be upfront about paying for it. I saw today that tax represents 5% of our energy bills, in Germnay its 48%. Also rhey have 10% VAT on food and of course higher income taxes.
ernie_lynch - MemberI don't know why you think controlled immigration means no immigration
It doesn't, and he didn't say it would- I don't know why you'd represent his comments that way.
But fundamentally everyone who deals with the UKVI, as myself and Kimbers do, will say the same thing- it will be massively harder. Visa procedures have become a political blunt instrument used not to tell people they [i]can't[/i] come here, but to make them feel that they shouldn't. Even the people we stand to benefit most from have been intentionally made to feel unwelcome. Costs have soared, timescales have slowed, processes become ever more involved and intentionally hard to understand, and change without warning or logic. The number of situations in which you're told you have to leave the country in order to reapply have gone up by orders of magnitude. People are turned away without good reason and treated like criminals based on factual errors and lack of rigour.
Perhaps this situation would be different. I think there's no likelihood that it would. Even while the government say "we're open to skilled workers" they would be working to deter them. The absurd targets this government has set for immigration are below the levels required for those immigrants we so desire, even if all other immigration is cut to zero.
I think you'll find it very hard to find anyone with experience of the UKVI that will say otherwise, unless paid to do so, and even then only sometimes.
Oh Jamby, if only there was a way we could be more like Germany, some sort of community we could be a part of perchance...
Northwind - MemberIt doesn't, and he didn't say it would- I don't know why you'd represent his comments that way.
I copied and pasted what he wrote. This is what I copied and pasted :
kimbers - MemberThere's also the issue of skilled labourer shortage, which could really get due if we leave the EU
And I responded with :
I don't know why you think controlled immigration means no immigration, or why you think immigration is the only solution to skills shortages.
To which he responded :
I agree ernie, but as pointed out from my own experiences, controls mean extra costs in time and money to the employer.
So you see he is perfectly capable of clarifying his position, and he did so, before your intervention.
Oh Jamby, if only there was a way we could be more like Germany, some sort of community we could be a part of perchance...
To be fair jambalaya has made the case for putting up taxes to pay for the NHS. I think we could leave the EU and put up taxes - don't you?
ernie_lynch - MemberI copied and pasted what he wrote.
Yes. And the part you copied and pasted doesn't support your suggestion that he thinks "controlled immigration means no immigration", nor did any part of his post. He didn't clarify his position; he didn't need to, his position was perfectly clear. Rather, he corrected your misinterpretation, or misrepresentation.
Yes. And the part you copied and pasted doesn't support your suggestion that he thinks "controlled immigration means no immigration".
Well in that case everyone was aware of this fact and it wasn't a problem.
I clearly misinterpreted what kimbers said. And he corrected my misinterpretation, or misrepresentation.
Oh Jamby, if only there was a way we could be more like Germany, some sort of community we could be a part of perchance...
To be fair jambalaya has made the case for putting up taxes to pay for the NHS. I think we could leave the EU and put up taxes - don't you?
To be fair, I was clearly ripping the piss...
In that case everyone was clearly taking the piss. As a staunch free-market Tory it's inconceivable that jambalaya would support raising taxes to pay for free universal healthcare.
This is very very old news ie 5 or so years old.
Also it does not change anything. NHS Property Solutions was set up when the PCT's were converted to CCG's. The theory being that it would help rationalise the community estate. Quite simply so far it is a shambles.
In theory by charging commercial rates then it will make Trusts think about running their estate more efficiently. However at the end of the day most NHS estate wouldn't be touched by the private sector as it is such shoddy standard.
Also just5minutes unfortunately your comments about bed need is completely wrong. All the data shows that bed requirement is shooting up in the next 5 yrs.
The Trust I work at would love to increase the number of beds/services and indeed car parking spaces. However the council will not allow us to add multi story car parks / build upwards.
Think your missing the point.
The rental increase was only announced in April 2016
I agree, not much physically is going to change - but financially, this is like shooting yourself in the foot, to see if it hurts..
The rental increase was only announced in April 2016
No it was known from the outset.
For the last couple of years or so Trusts having been asking NHS Prop what they will be charging, so that in hand the Trusts can go to their commissioner to ask for more funding, so that in hand the CCGs can go to DoH to ask for more funding.
I don't know about how the big trusts manage their estates, but I do know of at least one small rural GP practice that has had to close one of its branch surgeries due to rent increasing. So the policy has reduced access to healthcare for the elderly patients who are already isolated with poor public transport etc. This practice already provides a minibus to bring patients in to the main surgery but that can't service the whole area.
The idea of commercial rents for a service that is provided on £130 a year for an average of 6 appointments per person doesn't really stack up. How much would that service cost a commercial organisation to provide?
Here's a clue. Took dog to vets for routine booster last week. £38.
[i]but I do know of at least one small rural GP practice that has had to close one of its branch surgeries due to rent increasing.[/i]
Tell me I'm wrong, but aren't they a private business anyway and are just following standard 'commercial' practice?
A private business that is given a fixed contract sum to provide a service? yes.
In an open market where the provider of the service has any say in how much the sum is? No
Is the provider able to look elsewhere for a better deal in the market, amongst other commissioners of health care services? No
Is that sum the commercial value of the work that is done? No
See above. The total budget for primary care works out at around £130 per head per year. 340 million consultations a year and increasingly complex year on year.
You can pretend that NHS gp's are private providers of healthcare if you like.
Doesn't make it true though.
For the last couple of years or so Trusts having been asking NHS Prop what they will be charging, so that in hand the Trusts can go to their commissioner to ask for more funding, so that in hand the CCGs can go to DoH to ask for more funding.
Who can go to the government, who can just take it from the tax payers... ??
& not PropCo Ltd since they are £260million overspent already
[i]You can pretend that NHS gp's are private providers of healthcare if you like.
Doesn't make it true though[/i]
Eh? But on the whole GP's are private businesses, and do have control of their own budgets - just that the majority of their income comes from the Govt (obviously ignoring the 'Harley Street' types).
Ah, you've since edited your post - makes more sense now in what you are saying, but they're still private and no doubt make decisions based upon finances not just for 'social' reasons.
For the majority of GPs their employment status is "self-employed". This doesn't mean that they have much choice with regards who their clients are. The NHS has, for all intents and purposes, a completely monopoly over their clients. And the NHS stipulates what their prices are.
In that respect they are no more of a "private business" than a self-employed bricklayer who works for a bricklaying sub-contractor is a "private business".
Being self-employed rather than directly employed simply means than GPs can, if they so wish, and there is the demand, do a bit of private work.
But other than that the self-employed tag is something of a red herring.
b r
I didn't edit my post.
I can control what I spend money on. Whether I employ more doctors and less nurses, and vice versa etc. Who I use for telephone services, cleaning, maintenance etc. Just like a private business.
I have no control over how the government decided to fund general practice.
There is an absolute maximum income that is set by commissioners. Unlike private business. I can't just give everyone 2 flu jabs and upswell them a shingles jab at the same time.
The vast majority of the income is fixed in the contract sum that is £x per patient.
Increasing costs to commercial levels when income is fixed reduces the resource that is available to be spent on providing the service.
It's pretty simple really.
Having said all that, U.K. General practice has been very cheap historically because GP's are able to manage their own resources.
For instance a recent audit of the primary care estate where I work showed that practices in "lift" buildings (national project, management company, no control over costs etc) cost 4 x as much per square metre than gp owned or privately leased premises.
The vast majority of the income is fixed in the contract sum that is £x per patient.
Of course of you're good at playing the QOF game a bit more money sloshes around.
"Playing the qof game"? Nearly spat my Moët out there!
If only it was a game, as opposed to being part of the income stream that general practice relies upon to deliver a decent service.
We get about 20% of the value of the contract sum from qof, and we miss very few points.
Sure we could decide not to play the game, but we'd have to lose 3 full time GP's if we didn't get any qof income.
And it's included in the £130 per patient per year I mentioned earlier. It's not extra. You know, 2 months sky TV subscription for a year's worth of general practice....
And there is a maximum, controlled by government. That we rely on getting year on year out.
But every part of the NHS has quality payments. Cquins for trusts, quipp plans for CCGs. They're mostly about saving the NHS money rather than delivering improvements though.
so we need less hospitals and less beds in hospitals.
Not in acute care, we don't (still less mental health). ITU is like a nightclub on a friday night - one in, one out. Bed occupancy-wise, hospitals should be running at something like 80% capacity (i.e. with some degree of flexible slack) - and not rammed at 100%, like every major city infirmary is, right now, all across the country. And not all those sardine-like in-patients are "medically fit" elderly with nowhere to go for want of social care provision (though that is a very real problem) - they are acute admissions who [i]need[/i] to be there.
What the NHS [i]does[/i] need to get rid of, however, is revolving-door management consultancy con-artists. 👿
From private eye...
[img] 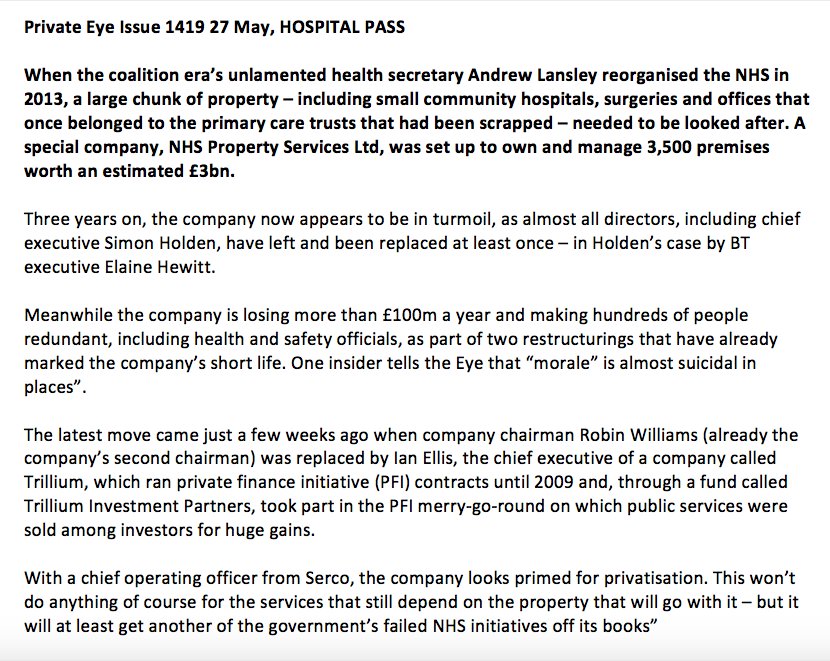 [/img]
[/img]
Worth a read, I hope
[url= http://campaign.r20.constantcontact.com/render?m=1102665899193&ca=94d77a5d-66d4-41a5-a1c7-11a989ae480e ]NHS Manager Blog[/url]
Very surprised that there's been no comment here on the expose by The Times journalist Billy Kenber concerning dodgy dealings in the NHS:
https://twitter.com/billykenber?ref_src=twsrc%5Egoogle%7Ctwcamp%5Eserp%7Ctwgr%5Eauthor
Edited to say that his reports are behind a paywall.
dodgy dealings in the NHS:
you mean the drug companies hiking prices?
Agreed it's a scandal, but someone has to look out for the shareholders!
This Peter Smith bloke is a bit of procurement guru and he's rightly angry, that the NHS has been so passive, given its virtual monopoly of demand..
[url= http://publicspendforumeurope.com/2016/06/06/rip-off-pricing-on-generic-drugs-a-failure-of-public-procurement/ ]Purchasing Blog[/url]
The thyroid world I live in has seen many patients write to their MP and the Health Secretary to point out that due to such massive cost increases in one product (Liothyronine) the CCGs are telling practices not to issue prescriptions.
This means that patients who've been successfully using this product to make them well are now forced to buy from overseas. There is no NHS substitute or alternative to this product. I recently bought some from overseas at a cost of £106 and that will only last a few months.
Will try and dig out some interesting links.
Procurement, yes indeed yet another problem. If you don't mind me saying a classic issue with over large bureaucratic state controlled organisation with a monopoly position. No one in admin is worried about the "company" going bust and them losing their job, no one is thinking about cost control as it doesn't matter - they'll just ask for a bigger budget and they know their customers have no choice so who really cares if the service provision deteriorates - its not their fault - it's the government not spending enough money.
Just seen this
inconceivable that jambalaya would support raising taxes to pay for free universal healthcare.
100% I would support substantial increases in taxes to pay for a better health service. However I also 100% believe that giving more money to the existing setup is NOT the way forward.
As I posted I knee ACL replacement surgery in both knees but NHS will not do it (trying very very hard not to) as I'm 53 (too old basically, was do you need ACL for, just walk slowly, don't run or do any active sports etc). I was warned about this by a lady which had dual replacement at 50 about how hard she had to fight to have it done.
cinnamon_girl - MemberThe thyroid world I live in has seen many patients write to their MP and the Health Secretary to point out that due to such massive cost increases in one product (Liothyronine) the CCGs are telling practices not to issue prescriptions.
Yup. Liothyronine has a monopoly supplier in the UK; they were bought out a couple of years ago and the new owners have used a loophole in the law to bang up the price by 5000%. No doubt this is the NHS's fault.
Maybe it should not be a monopoly supplier then ?
@samunkin thanks for that link - very interesting. Where I think it's spot on is that NHS will be there in your hour of need - it's an emergency service / critical care provider. The rest, not so much. As the piece says its about matching the money with the aspiration and that's what we should have a serious discussion about.
"inconceivable that jambalaya would support raising taxes to pay for free universal healthcare."100% I would support substantial increases in taxes to pay for a better health service. However I also 100% believe that giving more money to the existing setup is NOT the way forward.
Well of course not.........free universal healthcare? ........that's communism isn't it?
As a staunch free-market Tory I'm sure you would much rather private healthcare provisions. And if any government spending is required at all that it should go to private healthcare providers.
Because that idea works so well in the US of A.
Well when I say "works so well" I of course mean it is fabulously profitable. As we all know medical bills are the biggest cause of bankruptcy in the US.
jambalaya - MemberMaybe it should not be a monopoly supplier then ?
You're suggesting that the market has failed to deliver maximum value via competition? Inconceivable!
[quote=samunkim ]So you want Hospital Trusts to have started building multi-storey car-parks (which take decades to break ££s even) at a time when the NHS overspend is at an all time high ?
That surely depends on how you do the accounts. If construction of the multi-storeys is funded from selling off the land currently used for car parking for housing development (which is what seems to be the suggestion) then I doubt there is any problem with breaking even.
Interested to see that £130 per patient figure - I've gone years without getting my money's worth, though doing my best to make up for that this year (there's another accounting issue here - have been spending lots of time at the GP for an issue following surgery in the hospital which could probably have been solved in less than half the time if I'd had a follow up appointment with the surgeon - 9 months on I'm finally seeing the consultant again this week).