![]() You don't need to be an 'investor' to invest in Singletrack: 6 days left: 95% of target - Find out more
You don't need to be an 'investor' to invest in Singletrack: 6 days left: 95% of target - Find out more
You have this patient:
A 50 year old woman is admitted with severe abdominal pain and is vomiting blood due to a bleeding gastric ulcer; she undergoes an emergency laparotomy and partial gastrectomy. Second day post surgery she is in a flexed posture, is protecting her abdominal wound and is unable to expectorate. On auscultation she has reduced air entry and late inspiratory crackles in both lower zones and her arterial oxygen levels are low requiring her to be given oxygen therapy. She is also dehydrated as she is currently not permitted anything by mouth. She has a history of smoking 20 cigarettes per day up until her admission.
There is one tiny bit that I am unsure about. Why would the woman be dehydrated? Would she not be getting fluids intravenously? And would this not effect the thickness of any secretions she produced?
Long shot I know, but worth a punt i hope.
32:16 is what I'd recommend. My main question though, really is why? Is this your patient, or someone you know and you are questioning their treatment? Dehydration could be a result of infection, although more likely its die to restricted flu intake as fluid balance is very carefully monitored following surgery and bleeding.
Any bowel surgery, either upper GI or lower tends to leave people massively dehydrated, I mean massively...
It's not uncommon to give people 4-5-6 litres a day of fluid IV post bowel operations and yet they still appear 'dry'.
She is also very likely to have suffered for a few days pre-op; perfs often take a while to show up and so she may be fluid depleted from that as well.
Plus the effect of having a laparotomy; all that bowel and abdo contents exposed leads to fluid loss.
There will also be various effects due to her lack of nicotine and any usual meds, plus the required caution of the medics regarding fluid resus....
Please don't suggest saline nebs; it's witchcraft!
Crikey - Thanks.
They are wanting us to suggest saline nebs, thats the problem. Why do you think they're witchcraft? Wife is of similar opinion.
Meehaja - essay time. Got to get patho and treatment justification fitted into 750 words. Not being one to take the easy option I want to show that I've put a bit of thought into it.
It's a personal view, but I could never see that the kind of problem you are talking about is due to a lack of saline in someones lungs...
It's about proper, global, full-body hydration which does take time and careful monitoring to establish. Saline nebs are sometimes suggested on ITU, but I'm never convinced; it's a bit like moisturiser in the desert, if you get what I mean...
Proper hydration, with careful fluid balance and attention to urine output is the key; 30 mls an hour as a base, less than that over 3-4 hours would be a cause to review and either bump up the IV or look again for other causes.
Edit; and good pain relief to allow proper deep breathing and coughing.
If she has an epidural, unlikley because of the emergency surgery, then it's probably not working too well, or if she has a PCA, she's probably not able to use it effectively; maybe needs a look over by the pain team or on call anaesthetist or outreach team if you have one.
I want to show that I've put a bit of thought into it.
So you asked STW!
My thoughts are that once the gunk is in the lungs the only way to get it thinned it to send saline in via the airways to thin it out. A bit like sticking degreaser on the bike after a ride to get the gunk off. Whereas, we all know that it's much easier to keep the bike clear of gunk and get it clean afterwards if you give the bike a good spray of GT80 before you head out. If that makes sense to you.
Edit: plan would be to time treatment and pain relief so that they worked together, teach supported coughing, ACBT if they were bed bound or get them up and moving if they weren't.
OOOoooh you monkey!
Check out what I've said against reliable sources, I'm not sure my 'witchcraft' will go down well! 😉
I'm trying to speak from personal experience, and what you say is probably correct, but I'm never that convinced. It tends to be a sign that hydration or fluid replacement is not sufficient and should be a sign that you need to look more (and I hate this word) holistically at the patient.
Lots of the things physios see are not properly integrated into the whole MultiDisciplinaryTeam thing, so maybe go with your findings as a valuable contribution to the assessment of the patient. I wish our physios did TBH...
Crikey - although I'm choosing physio as a profession and love the subject, I think that a lot of the time physios are their own worst enemy. Spend way too much time trying to find their identity and role rather that just getting on with what a physio does.
Thanks for your help.
No worries! 😀
Huh - so this is for an essay then? Out of interest, what are you studying for?
Anyway, my take:
-Abdominal surgery = abdominal pain = lung base hypOventilation = basal atelectasis.....
-Clearly post surgery she'll not be feeling too chipper, and if her fluid balance is on the negative side, she'll be dehydrated.
-Saline nebs will help loosen the lung secretions (saline will 'draw' fluid across the lung mucosa to thin out the secretions), but as has been said, systemic hydration is important.
Or the short answer is - Bleep the med Reg and ask for help..."Hello, DrP here..." 😉
DrP
[i]Or the short answer is - Bleep the [b]med[/b] Reg and ask for help[/i]
Who will respond with 'Isn't that a surgical problem?'....
Then turn up anyway and steal any biscuits while checking out my staff nurses.....
DrP - Physio.
I don't know if it's a national or even just an English thing, but you know that all male physios have to be called Dave don't you?
We've got two who are and one who wishes he was...
[i]"Who will respond with 'Isn't that a surgical problem?'...."[/i]
Surgery's done, ergo, not the surgeon's problem! Or so it seems in my trust! 😉
DrP
You get a free Call Me Dave name badge with CSP registration.
Does this mean that physios can punt everything off onto medics?
[i]Surgery's done, ergo, not the surgeon's problem! Or so it seems in my trust![/i]
Ah, you need to make it the on-call anaesthetists problem, so 'pain' is the best call....
[i]Does this mean that physios can punt everything off onto medics?[/i]
Ooh no, just tell the staff nurse!
Oooh! Look at you and your fancy-dan jargon.
You still haven't told me what a VMO is! 😉
Viscous Membrane Overload?
Violently Modulated Occlusion?
Even i know that: Vastus Medialis Oblique....
[img] 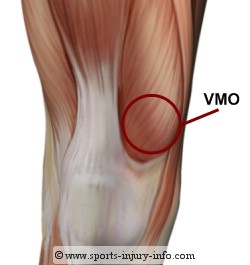 [/img]
[/img]
Is that the front or the back of the knee?
Is it in 1NF, 2NF or BCNF?
Alright, I've got one for you:
A patient has been running and he presents with a pain right on the inside of his shin bone just below half way up. Appears to be on the bone or on a tendon, but it's very localised. Like a bruise but he says he hasn't it, it just started on a run.
Compartment syndrome. Running too far too soon.
Next. 😉
Jesus! Tissue death?!
Not that bad!
Aye - your leg is going to fall off. Just rest it a bit and see if it clears up then start running again, but build mileage up more slowly. If it doesn't clear up seek medical help. You might want to do that anyway.
Well I had a hot bath, that seems to have helped 🙂
Really though, it just seemed strange that there'd be pain half way along a tendon. Nothing seems to start or end there or anything.
Bet you that it happens again on your next run. Unless that run is in 6 months time.
Lately the knot on the outside of the other calf has started hurting too.
Bloody running.
Running is bad for you.
Yeah, cycled for years and years and not a single non-impact related injury, and not even many of those.
Oh apparently the shin thing is just shinsplints. I wondered what that meant 🙂
Please don't suggest saline nebs; it's witchcraft!
Its exactly my first thought on this one
Or go back further into the past
[img]  [/img]
[/img]
I found this pic on an antiques site - gawd I am getting old - I used to use these when I first qualified.
TJ,I love those,particularly with added Friar's balsam.To OP I agree that the patient's problems are primarily medical,and she is probably very dry,but an ongoing pneumonia will not help,and in my limited experience( Charge nurse on resiratory care unit until last year) saline nebs can't hurt,and may have some positive benefit,but a patient that ill is unlikely to have a cough which will effectively clear their lungs wwhatever you do,and is highly unlikely to tolerate any physio which is vigorous enough to help.
Ian
P.S. however,if you know the required answer,why not just give it?
so, aside from some wifie you've not bothered to detail a pmh on, a set of gases about which the best you can say is they're hypoxic, no blood results - bilateral basal creps, i'll say it once again for the cheap seats BILATERAL BASAL CREPS - and the best treatment plan you can come up with is call a physio!?
and who said holistic? eh?
which is no comment on physios - the ones in my place are diamond. but none of them would entertain the above silliness. and fit in just fine with the whole mdt approach by the way. he said. smugly.
I should point out that this is the only information that we are given and that even i know that it's nothing like enough to give a decent response to.
jesmondingo - where's the fun in taking the easy option?
Well you'll be glad to know my shins are fine this morning but this annoying knot in the outside of my calf muscle is bothering me.
Dig your thumb into it and push as hard as you can stand for 6-10 seconds - see what that does. Might be best to get someone that doesnt like you to do it for you. Might need to repeat it a few times.
Let me know how you get on.
Did that last night a bit in the bath and out of it - helped in the short term. Not much change but I'll keep on.
On the few occasions I've had massages at races over the last few years they've found it each time and commented on it although it never bothered me til the running thing and even then only the last month or two. I think it goes back to some injury I had at school.
Weird huh.
Add some stretching into that too then. If it's an old injury like you say then it'll take a lot of work. Nothing to stop it going away with enough effort though.
I have one good stretch that I do, which is sitting with leg outstretched and reaching beyond my toes with my hands on the floor. That only stretches my back, shoulders and hamstrings tho. Perhaps it's time to do some research on stretching.. although I can't imagine how to stretch the outside of your calf!
If it's your calf muscle go find yourself a step, stand on your toes on it and lower yourself with a straight knee. I'd be guessing that the tightest bit would stretch first and that that would be your knot.
I stretch out my calves before running (or rather, after a short warmup run) and they are pretty flexible, that seems to miss the knot.
No idea then. Go get someone to check it out properly. Could be calcification or 101 other things.
to OP:
Has nobody mentioned positioning yet? FLEXED position, pain inhibition due to abdominal incision, poor basal expansion, been ventilated and anaesthetised in supine - collection of secretions etc, is analgesia correctly controlled? Immediate treatment approach would be get into a decent position to improve expansion, check fluid balance, chat with docs, saline nebs, flirt with nurses, eat chocolates, acbt with supported cough etc etc... re-auscultate, check to see if sats are improving,etc. If they're really crappy you can try the bird. Then liaise with docs again re: problems and get them to sort out fluid balance and any other issues.
Go get someone to check it out properly
I will, if it stays there. Just tried the stretching, could only get a bit of stretch in it by contorting my leg weirdly. I think perhaps the reason it's stayed there so long is that it doesn't get stretched out properly ever, it being on the side.